
PARADIGM-HF
What is the role of angiotensin-neprilysin inhibition in patients with HF?
Study design
Population
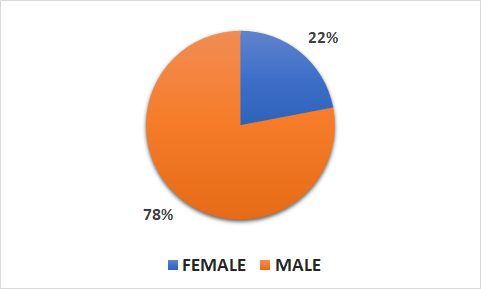
- 8442 patients (1832 female, 6567 male)
- Inclusion criteria: patients with class II, Ill, or IV HF and a reduced ejection fraction of < 40%
- Key exclusion criteria: symptomatic hypotension, a systolic BP of < 95 mmH at randomization, a serum potassium level > 5.4 mol/L at randomization, or a history of angioedema or unacceptable side effects during receipt of ACE inhibitors or ARBs
Interventions
- N=4187 sacubitril/valsartan (at a dose of 200 mg BID plus recommended therapy)
- N=4212 enalapril (at a dose of 10 mg BID plus recommended therapy)
Primary outcome
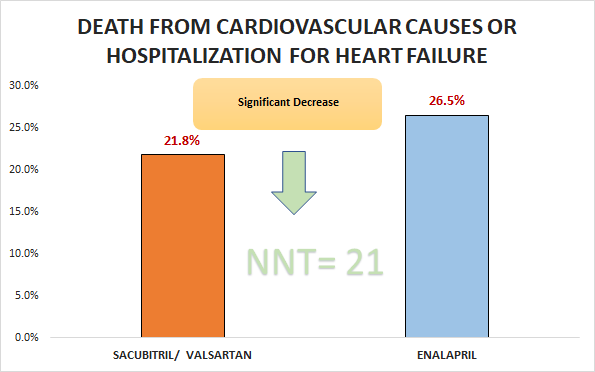
Significant decrease in death from cardiovascular causes or hospitalization for HF (21.8% vs. 26.5%; HR 0.8, 95% CI 0.73 to 0.87)
Secondary outcomes
- Significant decrease in death from any cause (17% VS. 19.8%; HR 0.84, 95% CI 0.76 to 0.93)
- Significant decrease in cardiovascular death (13.3% vs. 16.5%; HR 0.8, 95% CI 0.71 to 0.89)
- Significant decrease in hospitalization for HF (12.8% vs. 15.6%; HR 0.79, 95% CI 0.71 to 0.89)
Safety outcomes
- No significant difference in nonserious angioedema (0.2% VS. 0.1%).
- Significant differences in hypotension (14.0% VS. 9.2%), cough (11.3% vs. 14.3%), hyperkalemia (4.3% vs. 5.6%) and renal impairment (0.7% VS. 1.4%).
Conclusion
In patients with class lI, Ill, or IV HF and a reduced ejection fraction of ≤ 40%, sacubitril/valsartan was superior to enalapril with respect to death from cardiovascular causes or hospitalization for HF.