
NICE-SUGAR
What is the role of intensive glucose control in critically ill patients?
Study design

Population
- 6104 patients (2207 female, 3823 male)
- Inclusion criteria: adult medical and surgical patients admitted to the ICU who were expected to require treatment in the CU on ≥ 3 consecutive days
- Key exclusion criteria: age < 18 years, imminent death (cardiac standstill or brain death anticipated within 24 hours), ICU admission for treatment of DKA or hyperosmolar state, previous hypoglycemia without full neurological recovery, or at high risk of hypoglycemia
Interventions
- N=3054 intensive glucose control (with a target blood glucose range of 81-108 mg/dL)
- N=3050 conventional glucose control (with a target of
≤ 180 mg/dL)
Primary outcome
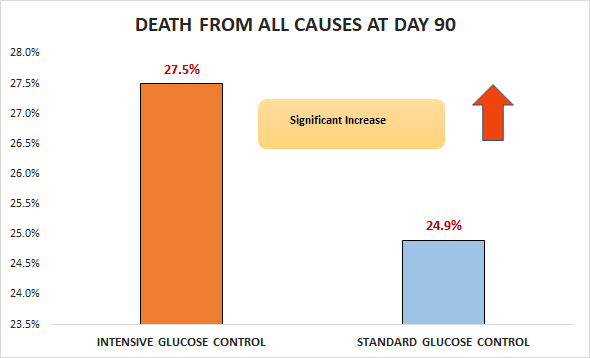
Significant increase in death from all causes at day 90 (27.5% vs. 24.9%; OR 1.14, 95% Cl 1.02 to 1.28)
Secondary outcomes
- No significant difference in RRT (15.4% VS. 14.5%; AD 0.9%, 95% CI-9 to 2.7)
- No significant difference in death at day 28 (22.3% vs.
20.8%; OR 1.09, 95% Cl 0.96 to 1.23)
Safety outcomes
Significant difference in severe hypoglycemia (6.8% vs. 0.5%).
Conclusion
In adult medical and surgical patients admitted to the ICU who were expected to require treatment in the ICU on ≥ 3 consecutive days, intensive glucose control was inferior to conventional glucose control with respect to death from all causes at day 90.