
EAST-AFNET 4
What is the role of early rhythm-control therapy in patients with AF?
Study design

Population
- 2789 patients (1293 female, 1496 male)
- Inclusion criteria: patients who had early AF diagnosed < 1 year before enrollment and cardiovascular conditions
- Key exclusion criteria: any disease that limits life expectancy to <1 year, pregnancy or breastfeeding, drug abuse, prior ablation or surgical therapy of AF, previous therapy failure on amiodarone, severe mitral valve stenosis, prosthetic mitral valve
Interventions
- N=1395 early rhythm control (treatment with antiarrhythmic drugs or AF ablation at an early time point)
- N=1394 usual care (following the 2010 ESC guidelines for AF treatment)
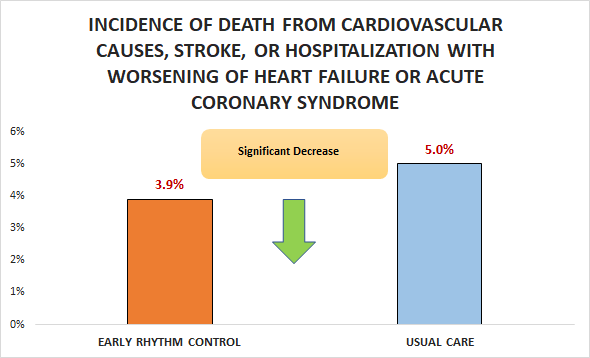
Primary outcome
Secondary outcomes
- No significant difference in the incidence of mean number of nights spent in the hospital (5.8 days / y vs.
5.1 days / Y; HR 1.08, 99% Cl 0.92 to 1.28) - No significant difference in change in European Quality of Life-5 Dimensions (EQ-5D) score at 2 years (-1 vs.
- 2.7; AD 1.07, 95% CI -0.68 to 2.82)
- Significant decrease in change in 12-Item Short-Form
- General Health Survey (SF-12) Mental score at 2 years
- (0.7 vs. 1.6; AD - 1.2, 95% CI-2.04 to -0.37)
Safety outcomes
- No significant difference in symptoms of LV function at 2 years and death.
- Significant difference in serious adverse events related to rhythm-control therapy (4.9% Vs. 1.4%).
Conclusion
In patients who had early AF diagnosed < 1 year before enrollment and cardiovascular conditions, early rhythm control was superior to usual care with respect to the incidence of death from cardiovascular causes, stroke, or hospitalization with worsening of HF or ACS.