
CAPE COD
Among patients with severe community acquired pneumonia requiring ICU or intermediate care unit admission, does hydrocortisone reduce the risk of all-cause mortality at 28 days when compared to placebo?
Study design
Multicenter, double-blind, parallel-group, randomized, controlled trial
Population
- Number of patients studied: 795
- Inclusion criteria: Aged ≥18 years, admitted to intensive care or intermediate care unit, diagnosis of community-acquired pneumonia within the first 48 hours of admission, study medication initiated within 24 hours after first severity criteria, severe disease with at least one severity criteria, on antibiotics, informed consent
- Exclusion criteria: Septic shock treated with vasopressors, aspiration as likely etiology, invasive ventilation in 2 weeks prior to admission, on antibiotics treating a respiratory infection for >7 days at the time of admission, certain pre-existing conditions, flu positive on PCR test, certain viral infections, myelosuppression, DNR, hypersensitivity to corticosteroids, needs corticosteroids or hydrocortisone for other reasons, on prednisone ≥15 mg/day or equivalent dosing of other corticosteroids for >30 days, enrolled in another trial with mortality as an endpoint, pregnant/breastfeeding, under guardianship
Interventions
- Experimental group: Hydrocortisone - 200 mg IV per day as a continuous infusion for 4-7 days, followed by a taper
- Control group: Placebo
Primary outcome
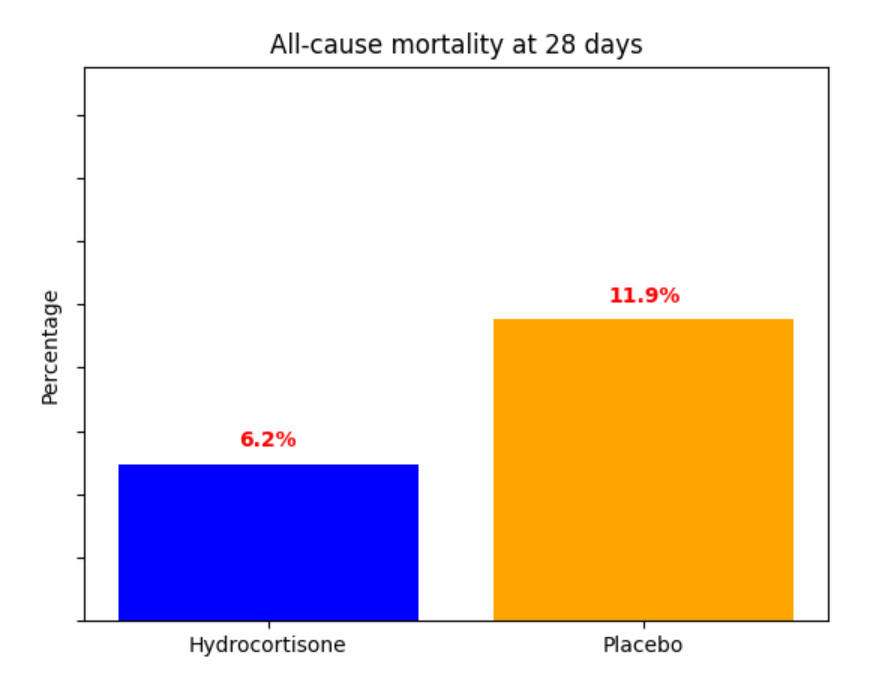
Significant difference
Secondary outcomes
All-cause mortality at 90 days, ventilation at 28 days, vasopressors at 28 days among those not receiving vasopressors at enrollment
Safety outcomes or Adverse Events
Serious adverse events: 70 events in the hydrocortisone group vs. 99 events in the placebo group
Conclusion
Hydrocortisone benefited severely ill pneumonia patients requiring ICU level care that did not have a contraindication to steroids, though this study excluded those who presented in septic shock requiring vasopressors. Consider hydrocortisone for admitted patients boarding in the ED who meet these inclusion criteri