
Apo-B Pathophysiology
Apolipoprotein B Superiority
The European Society of Cardiology/European Atherosclerosis Society states that apolipoprotein B (apoB) is a more accurate marker of cardiovascular risk than low-density lipoprotein cholesterol (LDL-C) and non-high-density lipoprotein cholesterol.
Mechanisms Governing ApoB Particles
The number of apoB particles determines cardiovascular risk. Mechanisms governing cholesterol mass within very low-density lipoprotein and low-density lipoprotein particles create the superior predictive power of apoB over LDL-C and non–high-density lipoprotein cholesterol.
Cardiovascular Risk and ApoB
The risk of cardiovascular disease relates more directly to the number of apoB particles in plasma than to the mass of cholesterol within them. The discordance between levels of apoB, LDL-C, and non-HDL-C underlies the superiority of apoB as a more accurate marker of cardiovascular risk.
ApoB Particles and Particle Number
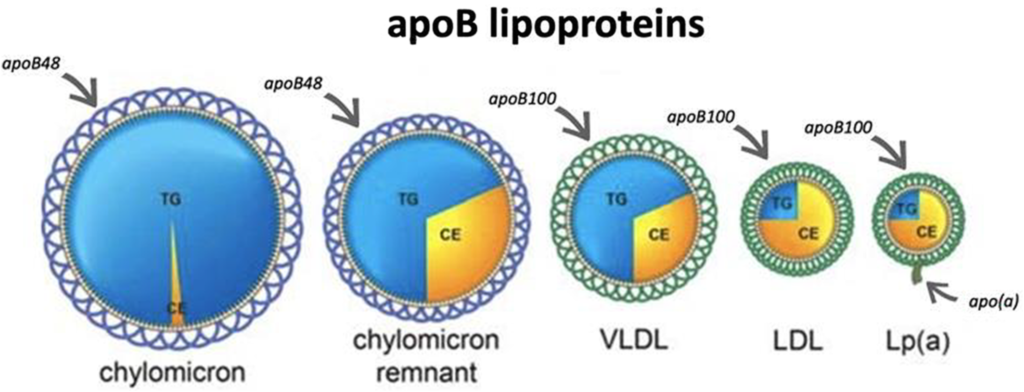
ApoB particles include chylomicron remnants, very low-density lipoprotein, and low-density lipoprotein particles. One molecule of apoB encircles each particle, making total plasma apoB an exact measure of the total number of apoB particles in plasma.
ApoB Dyslipoproteinemias
ApoB dyslipoproteinemias, such as dysbetalipoproteinemia, are disorders of apoB lipoprotein particle metabolism. Understanding these disorders can help improve diagnosis and simplify therapy.
VLDL Particle Variance
VLDL particles differ in size, with larger ones containing more triglycerides than smaller ones. Plasma triglycerides are not a measure of VLDL particle number. The mass of cholesterol per LDL particle also varies. Subclasses of LDL particles include LDL1, LDL2, and LDL3, each with different masses of cholesterol per particle. This variance in composition makes LDL-C an inexact and clinically unreliable measure of LDL particle numbers.
Pathophysiological Determinants of apoB Particles
Plasma apoB is effectively determined by the total number of VLDL and LDL particles. The number of these particles can increase due to increased production, decreased clearance, or a combination of both. The pathophysiology of apoB dyslipoproteinemia can be characterized by defects in clearance, production, or both.
Determinants of VLDL Particle Number
VLDL apoB particles are secreted by the liver, and their number in plasma is determined by production and secretion rates, which are influenced by various factors such as genetics, rates of triglycerides and cholesterol ester synthesis, and metabolic conditions. VLDL secretion rates are increased in patients with hypertriglyceridemia, abdominal obesity, insulin resistance, diabetes, and familial combined hyperlipidemia.
Determinants of LDL Particle Number
LDL particles are produced when triglycerides are removed from VLDL particles. The rate of VLDL particle production is the major determinant of LDL particle production. Factors affecting VLDL particle production also influence LDL particle production. The number of LDL particles in plasma is determined by their rate of production and clearance. The LDL receptor pathway is a critical component of LDL particle clearance and has been the focus of most research on LDL particle number regulation.
Limited LDL Particle Clearance Mechanisms
LDL receptor pathway saturation necessitates alternative mechanisms for LDL particle clearance. Nonspecific pathways, though unlimited in capacity, clear LDL particles less effectively.
Cholesterol Fluxes and LDL Particle Removal
The liver plays a central role in cholesterol fluxes, with multiple sources of cholesterol contributing to liver function. The LDL receptor pathway is one of several routes by which cholesterol is returned to the liver to maintain homeostasis.
Clearance vs. Production of LDL Particles
LDL particle number is influenced by the LDL receptor pathway and nonspecific pathways. The former is more effective but limited in capacity, while the latter is less effective but unlimited in capacity.
Impact of Varying Clearance and Production
Changes in clearance of LDL particles, production of LDL particles, or both can affect LDL apoB levels. Overproduction of LDL particles has a more dramatic impact on increasing LDL apoB than reducing clearance.
Variance in apoB Particle Composition
Triglyceride content in VLDL particles and cholesterol content in LDL particles can vary, leading to differences in correlations between plasma triglycerides and VLDL apoB or total apoB, and between apoB and LDL-C or non-HDL-C.
Pathophysiology of Discordance Between LDL-C/Non-HDL-C and apoB
Core lipid exchange, facilitated by cholesteryl ester transfer protein (CETP), is the primary mechanism for variance in cholesterol mass in apoB particles. Variability in cholesterol mass per apoB particle makes LDL-C and non-HDL-C imperfect surrogates of apoB.
apoB Dyslipoproteinemic Phenotypes
Distinctive patterns of dyslipoproteinemia can be characterized based on rates of VLDL and LDL particle production and clearance, and core lipid exchanges.
Pathophysiological Characteristics of the 4 Major apoB Dyslipoproteinemic Phenotypes
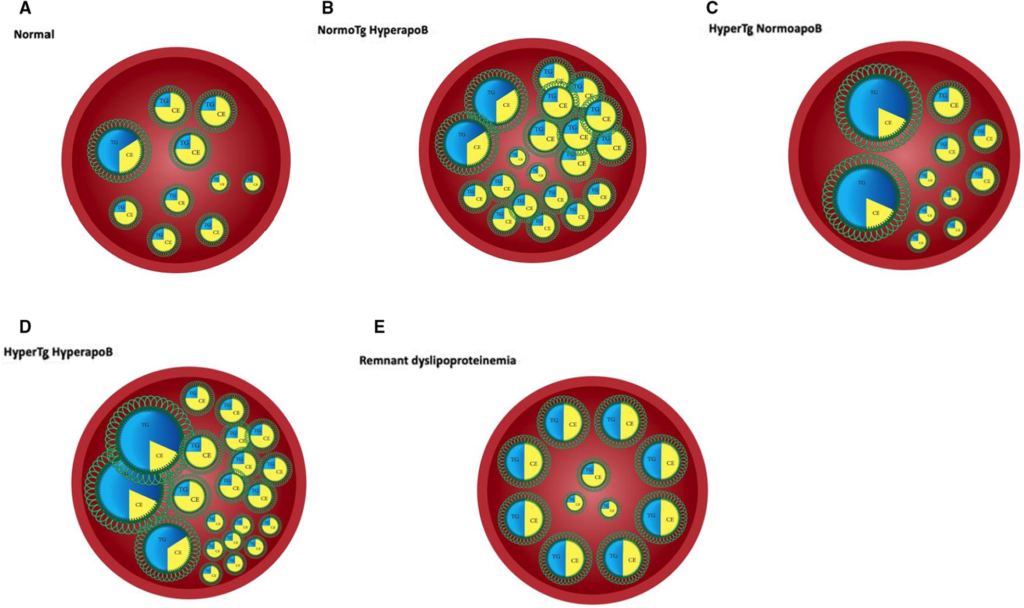
- Normal: Normal production and clearance rates of VLDL and LDL particles, resulting in normal levels of triglycerides, total cholesterol, and apoB.
- NormoTG HyperapoB: Normal plasma triglycerides and elevated apoB levels. Treatment may include statins, ezetimibe, PCSK9 inhibitors, or LDL apheresis.
- HyperTG NormoapoB: Elevated plasma triglycerides and normal apoB levels. Characteristic phenotype seen in mild-to-moderate hypertriglyceridemia.
- HyperTG HyperapoB: Elevated plasma triglycerides and apoB levels. Characteristic phenotype of familial combined hyperlipidemia.
These four apoB dyslipoproteinemic phenotypes help clinicians identify and treat dyslipidemia more effectively.
ApoB vs. Triglycerides in Therapy
Fibrates reduce triglycerides and VLDL apoB but only modestly reduce LDL apoB, resulting in a modest effect on total apoB. Statins, on the other hand, reduce VLDL and LDL apoB significantly, leading to better outcomes in clinical trials for cardiovascular health.
HyperTG HyperapoB
This condition is characterized by elevated apoB due to increased VLDL and LDL particle secretion. It's commonly found in people with abdominal obesity, type 2 diabetes, and premature coronary artery disease. It is also the hallmark dyslipoproteinemia in familial combined hyperlipidemia. Frontline therapy includes statins with apoB as the target, and additional treatments like ezetimibe or PCSK9 inhibitors may be required.
Dysbetalipoproteinemia
This condition features increased chylomicron and VLDL remnant particles, with low LDL particle numbers. The majority of affected individuals are homozygous for the apoE E2 isoform, but additional factors like obesity and diabetes may trigger the condition. Statins are the preferred initial therapy, with fibrates and niacin also being effective.
Summary
Cardiovascular risk correlates with apoB levels, which are determined by VLDL and LDL particle production and clearance rates. Triglycerides and LDL-C are not accurate markers of VLDL or LDL particle numbers, whereas apoB is. By integrating lipid and apoB information, clinicians can accurately diagnose various dyslipoproteinemias. Further research is needed to understand the processes regulating apoB concentrations and particle trapping within arterial walls, as these are key factors in atherosclerosis development.