
ALLHAT-ACEI
Is lisinopril superior to chlorthalidone in high-risk patients with HTN?
Study design
Population
- 24309 patients (11358 female, 12951 male)
- Inclusion criteria: patients ≥ 55 years of age with HTN and at least 1 other coronary heart disease risk factor
- Key exclusion criteria: history of hospitalized or treated symptomatic HF and/or known LV ejection fraction <35%
Interventions
- N=9054 lisinopril (a dose of 10-40 mg/day)
- N=15255 chlorthalidone (a dose of 12.5-25 mg/day)
Primary outcome
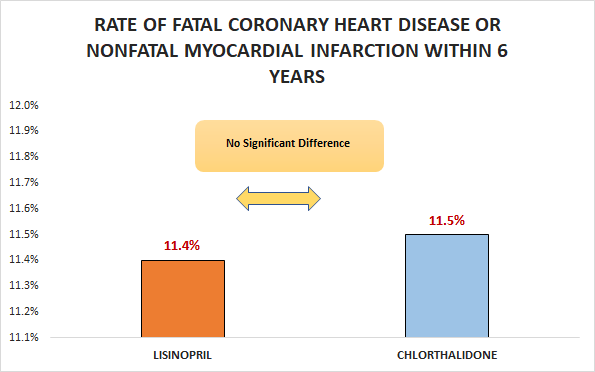
No significant difference in the rate of fatal coronary heart disease or nonfatal myocardial infarction within 6 years (11.4% vs. 11.5%; RR 0.99, 99% CI 0.91 to 1.08)
Secondary outcomes
- No significant difference in the rate of death from all causes within 6 years (17.2% vs. 17.3%; RR 1, 95% CI 0.94 to 1.08)
- No significant difference in the rate of coronary heart disease within 6 years (20.8% vs. 19.9%; RR 1.05, 95% CI 0.98 to 1.11)
- Significant increase in the rate of stroke within 6 years (6.3% vs. 5.6%; RR 1.15, 95% Cl 1.02 to 1.3)
Safety outcomes
No significant difference in hospitalization for gastrointestinal bleeding.
Conclusion
In patients ≥ 55 years of age with HTN and at least 1 other coronary heart disease risk factor, lisinopril was not superior to chlorthalidone with respect to the rate of fatal coronary heart disease or nonfatal myocardial infarction within 6 years.