
AFFIRM
What is the role of rhythm control strategy in patients with AF and a high risk of stroke or death?
Study design
Population
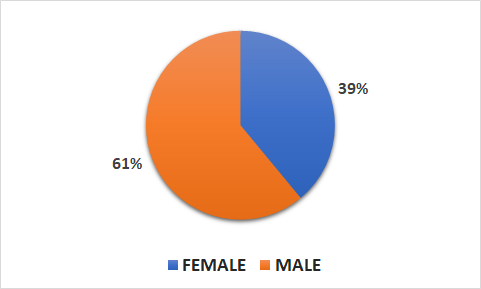
- 4060 patients (1594 female, 2466 male)
- Inclusion criteria: patients with AF and a high risk of stroke or death
- Key exclusion criteria: unsuccessful cardioversion, contraindication to certain therapies in the study, congestive HF, or renal abnormality
Interventions
- N=2033 rhythm control (antiarrhythmic drugs, cardioversion as necessary to maintain sinus rhythm)
- N=2027 rate control (target to control heart-rate control < 80 beats/min at rest and < 110 beats/min during six-minute walk test)
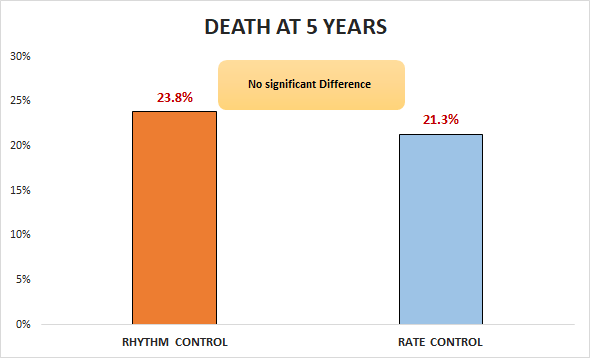
Primary outcome
Secondary outcomes
- No significant difference in death, disabling stroke, disabling anoxic encephalopathy, major bleeding, and cardiac arrest (32% vs. 32.7%; RR 0.98, 95% CI -0.97 to 2.93)
- No significant difference in CNS events (8.9% vs. 7.4%;
RR 1.2, 95% CI -23.34 to 25.74)
Safety outcomes
Significant differences in hospitalization during follow-up (80.1% vs. 73.0%, p < 0.001) and adverse drug effects leading to discontinuation (more common in rhythm-control group), including pulmonary events, gastrointestinal events, bradycardia, and prolongation of corrected QT interval (p < 0.001 for all comparisons).
Conclusion
In patients with AF and a high risk of stroke or death, rhythm control was not superior to rate control with respect to death at 5 years.