
ADVOR
In adult patients with acute decompensated heart failure characterized by volume overload, does acetazolamide in combination with loop diuretics as compared to loop diuretics alone improve time to successful decongestion within 72 hours?
Study design: Multicenter, double-blind, randomized, placebo-controlled trial
Population
- Number of patients studied: 519
- Inclusion criteria: Aged ≥18 years; admitted for acute decompensated heart failure and ≥1 of clinical sign of volume overload, oral maintenance diuretic for ≥1 month; known LVEF on imaging in the prior year.
- Exclusion criteria: Admission for known or suspected ACS; expected to require pressors; prior surgical correction for congenital heart disease; prior heart transplant or LVAD; on acetazolamide in the prior month; treatment with another proximal tubular diuretic, anticipated exposure to IV contrast or other nephrotoxin in the coming 3 days; SGLT2-inhibitor use; breastfeeding; incontinence
Interventions
- Experimental group: Acetazolamide 500mg IV daily, given with the first loop diuretic dose and for two additional days or until complete decongestion
- Control group: Placebo in addition to a doubling of their home loop diuretic dose, given as an IV formulation
Primary outcome
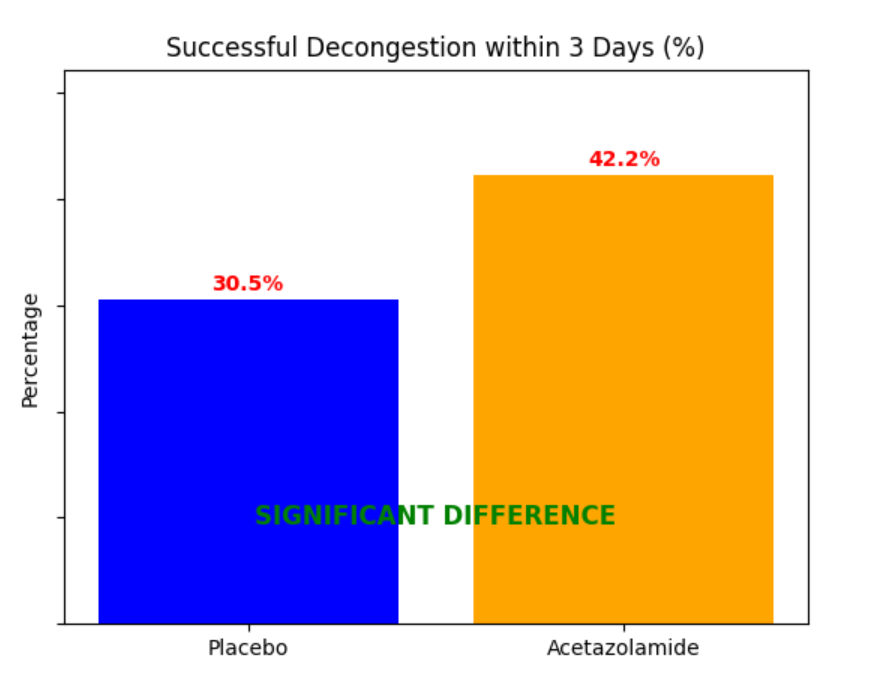
(30.5% in the placebo group vs. 42.2% in the acetazolamide group; RR 1.46, 95% CI 1.17-1.82; p<0.001)
Secondary outcomes: Hospital length of stay (9.9 days in the placebo group vs. 8.8 days in the acetazolamide group; RR 0.89, 95% CI 0.81-0.98; p=
0.02), weight loss at 72 hours (1.8 kg in the placebo group vs. 2.6 kg in the acetazolamide group; p<0.001), and proportion of patients with worsening renal function (24.6% in the placebo group vs. 15.8% in the acetazolamide group; RR 0.64, 95% CI 0.44-0.94; p=0.02).
Safety outcomes or Adverse Events: No significant difference in the number of serious adverse events between the two groups (22.4% in the placebo group vs. 20.5% in the acetazolamide group; RR 0.91, 95% CI 0.62-1.34; p=0.64).
Conclusion
Conclusion: In patients with acute decompensated heart failure characterized by volume overload, the addition of acetazolamide to loop diuretics resulted in a significantly higher rate of successful decongestion within 72 hours, reduced hospital length of stay, and decreased the proportion of patients with worsening renal function.